Findings: Spotting Acute Cholecystitis on POCUS: What to Look For, What Fools You, and Why it Matters
July 12, 2026 //
Caleb Neal, DO, MPH, and Tatiana Havryliuk, MD
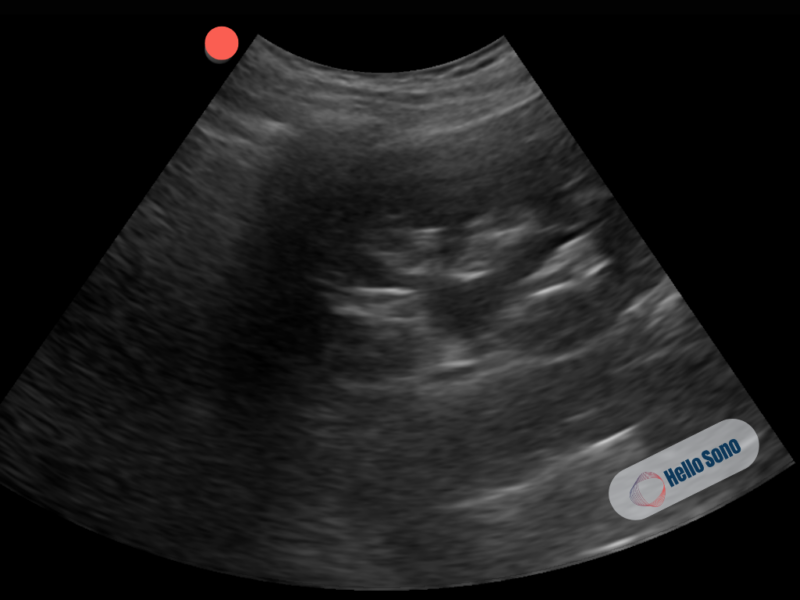
 Figure 1: Right upper quadrant ultrasound, with a longitudinal view of the gallbladder. Showing a hyperechoic focus with posterior acoustic shadowing (gallstone) in the back of the gallbladder. Anterior gallbladder wall is thickened to 5.1mm, and there is a small rim of pericholecystic fluid in the near field.
Figure 1: Right upper quadrant ultrasound, with a longitudinal view of the gallbladder. Showing a hyperechoic focus with posterior acoustic shadowing (gallstone) in the back of the gallbladder. Anterior gallbladder wall is thickened to 5.1mm, and there is a small rim of pericholecystic fluid in the near field.POCUS Findings
There are six classic ultrasound findings you're looking for in acute cholecystitis:1,6,8,11,12
- Gallstones: A bright (hyperechoic) focus inside the gallbladder with a dark shadow behind it, referred to as posterior acoustic shadowing which is the hallmark of a gallstone. Gallstones alone are not indicative of cholecystitis, there must be other signs of infection (included below), so gallstones alone are not included in the six classic findings of acute cholecystitis.
- Wall thickening: If the anterior gallbladder wall measures greater than 3mm, then this tells you the gallbladder is inflamed and possibly infected.
- Pericholecystic fluid: A thin dark stripe of fluid around the gallbladder, which is indicative of an inflammatory response to a gallbladder infection.
- Sonographic Murphy's sign: When the provider pushes the probe directly over the gallbladder, if the patient catches their breath from the tenderness, that's the ultrasound version of Murphy's sign.
- Stone-In-Neck (SIN) Sign: A stone impacted in the gallbladder neck or the cystic duct is the root cause of acute cholecystitis, and can be an important indicator if found on ultrasound.
- Gallbladder Distention (Hydrops): A normal gallbladder should have a transverse diameter of 4cm or less and a transverse diameter of 10cm or less. Anything greater than 4cm by 10cm is considered abnormal.
- Dilated Common Bile Duct (CBD): A normal CBD diameter is less than or equal to 6mm in people under 70, add 1mm to the CBD for every 10 years over 60 (i.e. 70-years-old = 7mm CBD is normal). Dilated CBD may indicate concomitant choledocholithiasis.
Put these together with the clinical picture, pain lasting more than 6 hours, fever, leukocytosis, and you've got acute cholecystitis diagnosed at the bedside.
What a Gallbladder without Cholecystitis Looks Like on POCUS
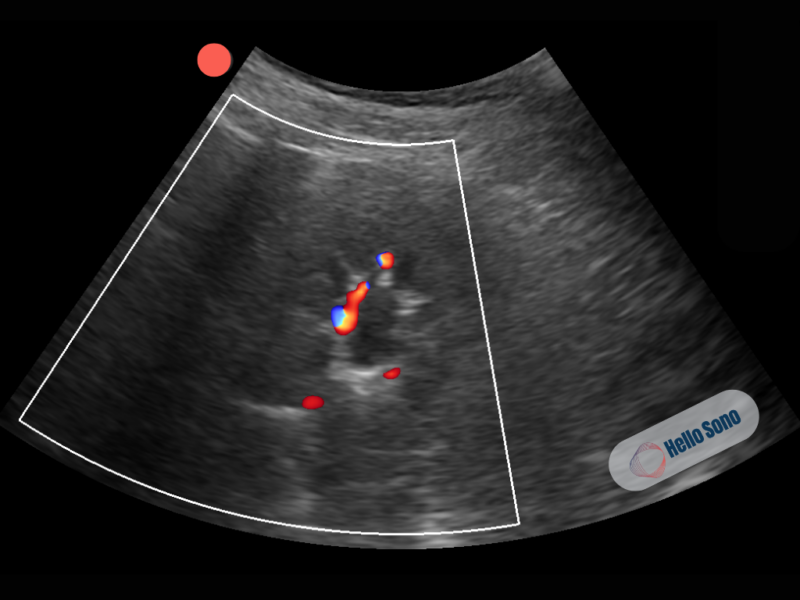
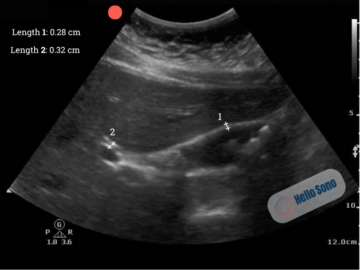 Figure 2: Ultrasound of a gallbladder in a longitudinal view: thin wall, anechoic (black) bile. Measurement 1 is the anterior gallbladder wall diameter, and measurement 2 is the CBD diameter. Since the gallbladder wall is less than 3mm and the CBD diameter is less than 6mm, both are considered normal. Hyperechoic stones with posterior acoustic shadows are seen.
Figure 2: Ultrasound of a gallbladder in a longitudinal view: thin wall, anechoic (black) bile. Measurement 1 is the anterior gallbladder wall diameter, and measurement 2 is the CBD diameter. Since the gallbladder wall is less than 3mm and the CBD diameter is less than 6mm, both are considered normal. Hyperechoic stones with posterior acoustic shadows are seen.
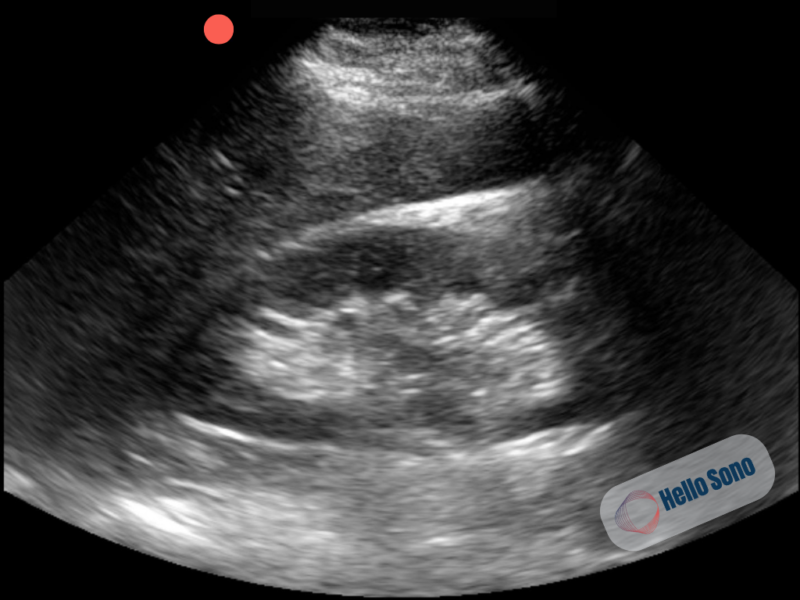
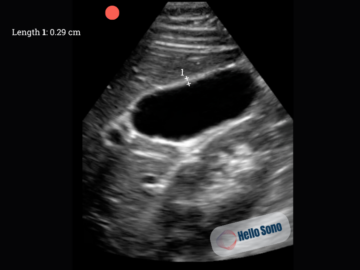 Figure 3: Ultrasound of a normal gallbladder in a transverse view with a thin GB wall and anechoic bile with no stones visualized. Measurement 1 is the anterior gallbladder wall, which is less than 3mm and therefore within normal limits.
Figure 3: Ultrasound of a normal gallbladder in a transverse view with a thin GB wall and anechoic bile with no stones visualized. Measurement 1 is the anterior gallbladder wall, which is less than 3mm and therefore within normal limits.Before you can spot what's wrong, you need to know what's normal. A healthy gallbladder on ultrasound looks like:1,6
- A thin-walled, pear-shaped structure filled with dark (anechoic) bile
- The wall should be less than 3mm thick
- No bright foci or shadows inside the lumen
- The gallbladder sits just below the liver edge, use the liver as your acoustic window to find it
- No fluid around the outside of the gallbladder
Why This Matters: Biliary Colic vs. Cholecystitis
Here's the clinical question that POCUS helps answer: Is this just another episode of biliary colic or has this patient crossed the line into acute cholecystitis?
The dividing line is mostly about time and inflammation:
- Biliary colic occurs when a stone temporarily blocks the cystic duct. The pain peaks within about an hour and usually resolves within 5 hours. The gallbladder isn't inflamed, it's just irritated. On ultrasound, you'll see stones, but the wall looks normal and there's no pericholecystic fluid.4,10
- Cholecystitis happens when that blockage doesn't clear. The gallbladder stays obstructed, gets inflamed, and starts to swell. Pain lasts more than 6 hours. On ultrasound, you see stones PLUS secondary signs of inflammation: wall thickening, enlarged gallbladder, a stone-in-neck, pericholecystic fluid, a dilated CBD, and a positive sonographic Murphy's sign.1,4,6,10,11,12
This is why history matters so much. A patient who says "I've had this pain for 2 hours that’s coming and going and it's getting better" is a very different story from "this started 10 hours ago and it's only getting worse."
If your patient has had previous episodes of biliary colic, check out the Hello Sono blog on cholelithiasis for a deeper dive into stone detection and biliary colic management: https://www.hellosono.com/hello-sono-blog/pocus-gallstones-ruq-pain-diagnosis
Common Pitfalls
Gallbladder ultrasound is one of the most reliable bedside exams out there, but there are a few traps that catch people.
Pitfall #1: Wall thickening that isn't cholecystitis
This is the big one. A thick gallbladder wall does NOT automatically mean cholecystitis. Other conditions cause the wall to thicken:9
- Heart failure: right-sided congestion causes venous engorgement of the gallbladder wall
- Liver disease/cirrhosis/portal hypertension: same mechanism, venous congestion
- Acute hepatitis: diffuse inflammation of the liver can thicken the gallbladder wall
- Hypoalbuminemia (nephrotic syndrome, malnutrition): low protein causes edema everywhere, including the gallbladder wall
- Ascites: fluid surrounding the gallbladder can make the wall appear thickened
- Recent eating: a contracted, postprandial gallbladder can make the wall look artificially thick
The key is context. Wall thickening in a patient with right upper quadrant pain, stones, and a positive sonographic Murphy's sign means cholecystitis. Wall thickening in a patient with known cirrhosis and ascites but no focal tenderness is most likely not cholecystitis.
Pitfall #2: Sludge vs. stones
Biliary sludge (thick, echogenic bile) can look like stones at first glance. The difference? Sludge doesn't cast a posterior acoustic shadow, and it layers dependently (meaning it settles to the bottom) without the sharp, bright edges of a true stone. Sludge can be seen in cholecystitis, but it can also show up in patients who are fasting, on TPN, or critically ill, so it's not specific.
Pitfall #3: Duodenal artifact
Gas in the duodenum, which sits right next to the gallbladder, can create bright echoes that mimic stones. The difference is that duodenal gas moves with peristalsis, doesn't cast a clean shadow, and isn't inside the gallbladder lumen. Scanning in multiple planes can help to sort this out.
Pitfall #4: Missing stones in the gallbladder neck
Stones love to hide in the neck of the gallbladder, the narrowest part that leads to the cystic duct. If you only scan in a long axis, you might miss them. Always rotate to a short axis and fan through the neck carefully.
Pitfall #5: The "WES" sign
When the gallbladder is packed full of stones, you may not see the lumen at all. Instead, you'll see three layers: the gallbladder Wall, the bright Echo of the stones, and the dark Shadow behind them. This is the WES sign (Wall-Echo-Shadow), and it means the gallbladder is full of stones. Don't mistake it for bowel gas.
Gallbladder Wall Changes Can Evolve Over Time
Furthermore, cholecystitis is a dynamic process, and the ultrasound findings evolve over time. A recent study found that among patients who initially had no gallbladder wall changes on their first ultrasound, nearly 20% developed wall thickening on repeat imaging a median of 4 hours later. Patients who developed these changes had longer hospital stays and were more likely to have confirmed cholecystitis.7
If your clinical suspicion is high but the initial POCUS only shows stones without wall thickening, don't completely dismiss cholecystitis. The inflammatory changes may not have had time to develop yet. Consider serial exams, further workup, or immediate outpatient follow-up if the clinical picture doesn't add up.
Evidence: How Good Is POCUS for Cholecystitis?
POCUS isn't perfect for cholecystitis, no single test is, but it is remarkably useful when combined with clinical judgment. A 2024 meta-analysis pooled data from seven studies (1,464 patients) and found that POCUS had a pooled sensitivity of 86% and specificity of 92% for gallbladder disease overall.12 Other studies also found POCUS to be an integral part of the work-up for cholecystitis:
- Gallstone detection by POCUS: Sensitivity 90–96%, specificity 88–96%1
- Overall ultrasound accuracy for cholecystitis: Sensitivity ~81%, specificity ~83%4
- Gallstones + sonographic Murphy's sign: Positive Predictive Value (PPV) of 92%10
- Gallstones + wall thickening: PPV of 95%10
- No stones + negative sonographic Murphy's sign: Negative Predictive Value (NPV) of 95%10
- CT vs. ultrasound: A 2024 meta-analysis found comparable diagnostic performance between CT and ultrasound for cholecystitis (CT sensitivity 84% vs. US 79%, p = 0.44), with 82% concordance between the two modalities.2
One study offered an important counterpoint. In their single-center study of 147 patients, POCUS had a sensitivity of only 40% for cholecystitis, significantly lower than the pooled estimates.11 Their study highlighted that POCUS accuracy is operator-dependent and that clinical findings and lab data should always be part of the diagnostic equation.
The Bedside Sonographic Acute Cholecystitis (SAC) Score combines three clinical findings (postprandial symptoms, RUQ tenderness, and Murphy's sign) with two POCUS findings (gallstones and wall thickening) into a single score. A SAC score below 2 has 100% sensitivity (great for ruling out), while a score of 7 or above has 96% specificity (great for ruling in).5
The bottom line: POCUS won't catch every case of cholecystitis, but when you combine what you see on ultrasound with the clinical picture, it's a remarkably effective bedside tool. A recent large multicenter study reinforced that POCUS should not be used as a standalone diagnostic test, it works best when integrated with clinical and laboratory data.8 And there's a practical throughput benefit too: bedside POCUS by emergency physicians decreases length of stay by 7% overall and up to 15% during evening and overnight hours compared to waiting for a radiology ultrasound.1
Case Resolution
Given the combination of persistent right upper quadrant pain, positive Murphy's sign, leukocytosis, and POCUS findings of gallstones with wall thickening and pericholecystic fluid, the provider diagnoses acute cholecystitis at the bedside.
The patient is made NPO, started on IV fluids and antibiotics, and surgery is consulted. She undergoes laparoscopic cholecystectomy the following morning, within 24 hours of diagnosis. Surgical pathology confirms acute cholecystitis. She's discharged home the next day.
Impact of POCUS
In this case, bedside ultrasound:
- Confirmed the diagnosis in minutes: no waiting for radiology availability
- Accelerated the surgical consultation: the surgeon was called before the formal ultrasound was even ordered
- Reduced time to definitive care: early cholecystectomy within the optimal 1–3 day window
- Avoided unnecessary additional imaging: no CT was needed
- Improved patient experience: faster answers, faster treatment, and shorter hospital stay
Conclusion
Acute cholecystitis is one of the most common surgical emergencies, affecting approximately 200,000 people in the US each year.4 POCUS puts the diagnosis in your hands. By combining gallstone detection with secondary signs of inflammation (wall thickening, pericholecystic fluid, sonographic Murphy's sign) and correlating with the clinical picture, you can make a confident bedside diagnosis that changes management in real time.
The key is remembering that no single finding rules cholecystitis in or out. It's the combination of what you see, what the patient feels, and what the labs show that gets you to the answer. And when the picture is clear, don't wait, get surgery involved early. The evidence is unambiguous: early cholecystectomy wins.
References
- American College of Emergency Physicians (ACEP) Sonoguide. Gallbladder. www.acep.org. https://www.acep.org/sonoguide/basic/gallbladder
- de Oliveira GS, Torri GB, Gandolfi FE, et al. Computed tomography versus ultrasound for the diagnosis of acute cholecystitis: a systematic review and meta-analysis. Eur Radiol. 2024;34(11):6967-6979. doi:10.1007/s00330-024-10783-8
- Fugazzola P, Podda M, Tian BW, et al. Clinical Update on Acute Cholecystitis and Biliary Pancreatitis: Between Certainties and Grey Areas. EClinicalMedicine. 2024;78. doi:10.1016/j.eclinm.2024.102929
- Gallaher JR, Charles A. Acute Cholecystitis: A Review. JAMA. 2022;307(9):916-924. doi:10.1001/jama.2022.2350
- Graglia S, Shokoohi H, Loesche MA, et al. Prospective Validation of the Bedside Sonographic Acute Cholecystitis Score in Emergency Department Patients. Am J Emerg Med. 2021;44:36-40. doi:10.1016/j.ajem.2020.12.081
- Hello Sono. POCUS Implementation & Credentialing Support. POCUS Implementation & Credentialing Support. Published November 19, 2025. https://www.hellosono.com/hello-sono-blog/pocus-gallstones-ruq-pain-diagnosis
- Ivanov D, Cannata D, Chin KA, et al. Evolution of Secondary Findings in Acute Cholecystitis: A Temporal Analysis From Point-of-Care Ultrasound to Subsequent Imaging. J Emerg Med. 2025. doi:10.1016/j.jemermed.2025.03.009
- Nipitkul N, Kotnarin R. Agreement between point-of-care ultrasonography and the Tokyo guidelines 2018 for acute cholecystitis (PACED study). CJEM. 2026;28(6):588-594. doi:10.1007/s43678-026-01161-y
- Rosselli, M., Radzina, M. and Lim, A.K.P. (2023). Ultrasound of the Biliary System. In Liver Ultrasound (eds A.K.P. Lim and M. Rosselli). https://doi.org/10.1002/9781119612650.ch6
- Strasberg SM. Clinical practice. Acute calculous cholecystitis. N Engl J Med. 2008;358(26):2804-2811. doi:10.1056/NEJMcp0800929
- Wehrle CJ, Talukder A, Tien L, Parikh S, Devarakonda A, Holsten SB, Fox ED, Lawson A. The Accuracy of Point-of-Care Ultrasound in the Diagnosis of Acute Cholecystitis. Am Surg. 2022 Feb;88(2):267-272. doi: 10.1177/0003134821989057. Epub 2021 Jan 31. PMID: 33517707.
- Wu X, Li K, Kou S, Wu X, Zhang Z. The Accuracy of Point-of-Care Ultrasound in the Detection of Gallbladder Disease: A Meta-analysis. Acad Radiol. 2024 Apr;31(4):1336-1343. doi: 10.1016/j.acra.2023.09.029. Epub 2023 Oct 12. PMID: 37838525.
About the Authors
Dr. Caleb Neal is an emergency medicine resident in NYC passionate about POCUS.
Dr. Tatiana Havryliuk is an emergency physician with over 15 years of clinical POCUS experience, former Emergency Ultrasound Director at The Brooklyn Hospital Center (NY), and founder of Hello Sono. She is dedicated to integrating POCUS into primary care to enhance diagnostic accuracy and patient safety.
LinkedIn: https://www.linkedin.com/in/tatiana-havryliuk-md/
Email: [email protected]
*POCUS images and graphics provided courtesy of Hello Sono.