Findings: Do You Need a CT? POCUS in First-Time Renal Colic
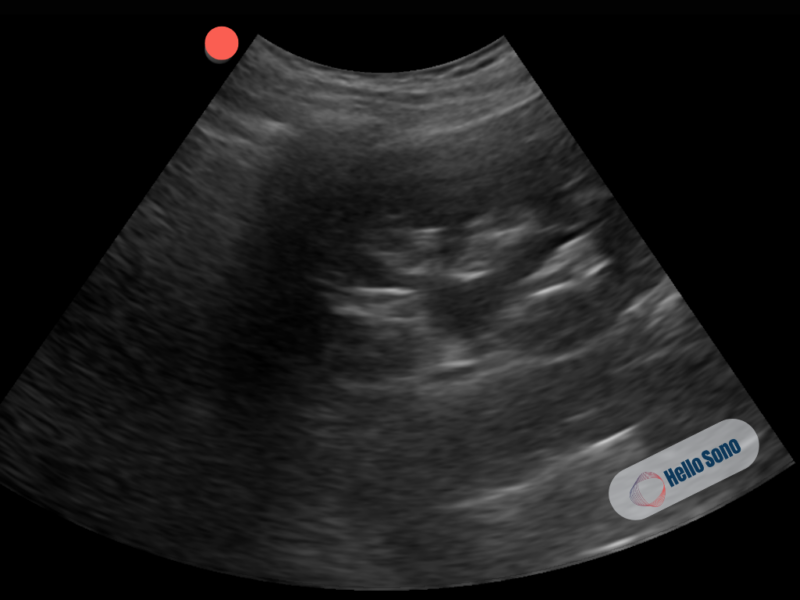
Figure 1: Coronal view of the left kidney showing mild hydronephrosis (anechoic dilation of the renal pelvis) without perinephric fluid or dilation of the calices.
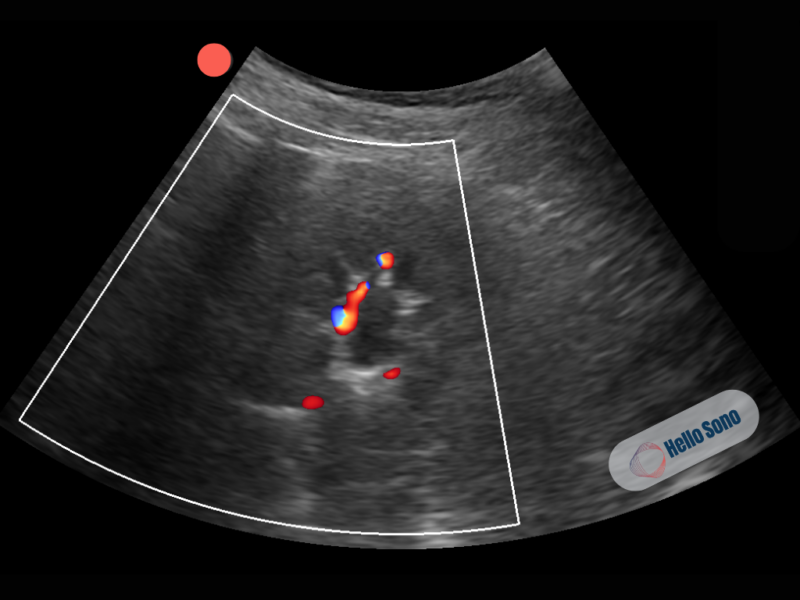
Figure 2: Transverse view of the left kidney demonstrating mild hydronephrosis. A small central anechoic area represents dilation of the renal pelvis. Color Doppler shows vascular flow in the renal parenchyma with absence of flow in the collecting system, confirming that this structure is not vascular and is consistent with hydronephrosis.
POCUS Findings:
The ultrasound demonstrates mild hydronephrosis of the left kidney, characterized by:
- Small, anechoic dilation of the renal pelvis
- No extension into the calyces
- Preserved cortical thickness
- On transverse view with color Doppler, vascular flow is seen in the renal parenchyma, with no flow in the central anechoic region, confirming fluid within the collecting system rather than vascular structures
These findings are consistent with early urinary obstruction, most commonly due to a ureteral stone. It is important to note that POCUS often does not directly visualize the ureteral stone and instead identifies secondary signs of obstruction, such as hydronephrosis.
What a Normal POCUS Should Look Like:
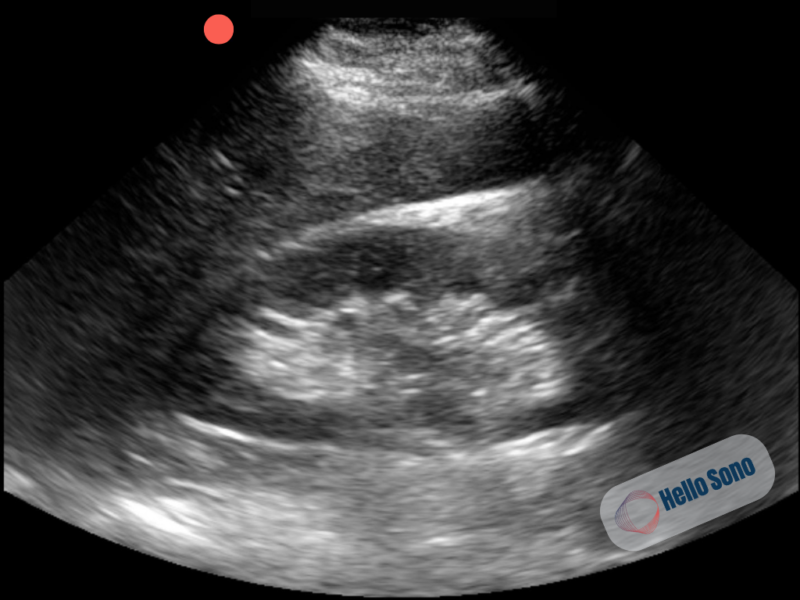
Figure 3: Coronal view of the patient's left kidney showing no dilation of the pelvis or calyces.
In a normal kidney, the collecting system is collapsed and not visualized as a fluid-filled structure. Normal renal POCUS show:
- No visible dilation of the renal pelvis
- Central sinus appears echogenic rather than anechoic
- Preserved corticomedullary differentiation
Common Pitfalls:
Several findings can mimic or represent physiological hydronephrosis on renal POCUS. Recognizing these helps avoid overcalling clinically significant obstruction.
Renal Cysts
Simple cysts appear as well-circumscribed, anechoic structures within the renal parenchyma. Unlike hydronephrosis, they are focal and do not communicate with the collecting system. A key step is to follow the anechoic area in multiple planes. Hydronephrosis will appear connected and extend into the renal pelvis and calyces, whereas cysts remain isolated.
Vascular Structures
Renal vessels can also appear anechoic. Color Doppler can help to differentiate these. True hydronephrosis will show no flow, while vascular structures will demonstrate internal flow.
Prominent Medullary Pyramids
Renal pyramids can appear hypoechoic and may be mistaken for hydronephrosis. Unlike hydronephrosis, they are discrete, symmetric structures that do not connect to the renal pelvis and are surrounded by normal renal parenchyma. Following the area in multiple planes helps confirm that there is no communication with the collecting system.
Physiologic Hydronephrosis
Not all hydronephrosis reflects a pathologic obstruction. Mild dilation of the collecting system can occur due to functional or transient impedance of urine flow, including:
- Bladder distention, which can cause back pressure and mild, often bilateral hydronephrosis
- Pregnancy, where hormonal and mechanical factors lead to physiologic dilation in 70% to 90% of pregnant patients
Interpreting these findings requires context. Assess the bladder for distention, evaluate both kidneys, and correlate with the clinical presentation. In contrast, unilateral hydronephrosis in a patient with acute colicky flank pain is more concerning for an obstructing stone.
When Should CT and Escalation of Care Be Considered:
- Age ≧ 60
- Fever (currently or at home)
- Intractable pain
- Abnormal vitals after pain control
- Vomiting not relieved with antiemitics
- Inability to urinate
- Concern for aortic pathology
- Urinalysis demonstrates infection
- Severe hydronephrosis
Moderate hydronephrosis on POCUS suggests a larger stone. If the patient’s pain is well controlled and there are no high-risk features the patient can receive a nonemergent CT to confirm stone size and outpatient follow up.
Evidence
POCUS sensitivity for hydronephrosis is 84% (range 73–92%) and specificity is 79% (range 59–83%) for suspected renal colic. [1-2] The sensitivity of POCUS increases to 94.4% for moderate to severe hydronephrosis. [3] An ultrasound-first approach reduces time to diagnosis, cumulative radiation exposure, and cost compared with CT. [4-5] Across 29 clinical scenarios for suspected renal colic, CT was recommended in only 24% of scenarios, while ultrasound alone or no further imaging was sufficient in 76% of cases.[5]
Beyond diagnostic accuracy, it is important to consider the downstream cost and resource implications of how patients with renal colic are managed. Chadwick et al. found that 7.9% of emergency department visits for urolithiasis were potentially avoidable, defined as visits that did not result in intervention, admission, or specialty referral. This translated to nearly $95 million in annual potentially avoidable costs across just two states (Florida and New York). [6]
Case Resolution:
Given the patient’s stable presentation, absence of infection, and only mild hydronephrosis on POCUS, the provider diagnoses uncomplicated renal colic.
The patient is treated with oral analgesics, hydration guidance, and return precautions. He is discharged home with outpatient follow-up and instructions to return for fever, worsening pain, inability to tolerate PO, or decreased urine output.
No ED transfer or CT imaging is performed.
Impact of POCUS:
POCUS directly influenced both clinical decision-making and resource utilization in this case:
- Avoided unnecessary ED transfer in a stable patient
- Reduced radiation exposure by deferring CT in a young patient
- Provided immediate diagnostic confidence at the bedside
- Streamlined care with same-visit decision-making
- Improved patient experience by avoiding prolonged workups
- Reduced overall costs
Beyond clinical impact, integrating POCUS into clinical workflows enables appropriate reimbursement when supported by proper credentialing, documentation, and quality assurance. For a practical framework, download the Hello Sono POCUS Billing Readiness Checklist.
Conclusion:
Renal POCUS is a powerful tool in the evaluation of suspected renal colic, particularly in urgent care and primary care settings. In young, stable patients with classic symptoms, identifying mild hydronephrosis at the bedside can support a safe, CT-free, outpatient management strategy.
Using POCUS, clinicians can risk stratify patients in real time, supporting appropriate outpatient management while reducing unnecessary imaging, lowering costs, and improving patient-centered care.
References:
- Lee S, Kim J, Park Y, et al. Test characteristics of point-of-care ultrasonography in patients with renal colic. Ultrasound J. 2023;15:27.
- Pathan SA, Mitra B, Mirza S, et al. Emergency physician interpretation of point-of-care ultrasound for identifying and grading hydronephrosis in renal colic. Acad Emerg Med. 2018;25(10):1129-1137.
- Wong C, Teitge B, Ross M, et al. Accuracy and prognostic value of point-of-care ultrasound for nephrolithiasis: systematic review and meta-analysis. Acad Emerg Med. 2018;25(6):684-698.
- Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N Engl J Med. 2014;371(12):1100-1110.
- Moore CL, Carpenter CR, Heilbrun ME, et al. Imaging in suspected renal colic: systematic review and consensus. Ann Emerg Med. 2019;74(3):391-399.
- Chadwick SJ, Dave O, Frisbie J, Scales CD Jr, Nielsen ME, Friedlander DF. Incidence and cost of potentially avoidable emergency department visits for urolithiasis. Am J Manag Care. 2023 Nov 1;29(11):e322-e329. doi: 10.37765/ajmc.2023.89458. PMID: 37948652.
About the Author
Dr. Havryliuk is an emergency physician with over 15 years of clinical point-of-care ultrasound (POCUS) experience, a past Emergency Ultrasound Director at Brooklyn Hospital in NY, and the founder of Hello Sono. She is on a mission to empower clinicians with POCUS to take better and more efficient care of their patients by addressing two key barriers, lack of competency and infrastructure.
LinkedIn: https://www.linkedin.com/in/tatiana-havryliuk-md/
Email: [email protected]
*POCUS images and graphics provided courtesy of Hello Sono.