RUQ Pain: Expedited Work-Up with POCUS
Case Presentation
A 42-year-old female presents to her primary care clinic with intermittent, crampy abdominal pain for four months. The pain typically follows fatty meals, occasionally radiates to her right shoulder, and can last for several hours. She denies fever, vomiting, or diarrhea. Vital signs are normal. On exam, she has mild tenderness to palpation in the right upper quadrant without rebound or guarding. There is no jaundice, and laboratory studies, including AST and ALT, are within normal limits.
Given the postprandial nature and location of pain, the clinician performs a right upper quadrant point-of-care ultrasound (POCUS) to evaluate for gallstones.
A representative image is shown below (Image 1). The patient does not exhibit a sonographic Murphy’s sign.
What do you see, and what’s the diagnosis?

POCUS Findings
POCUS reveals hyperechoic structures within the gallbladder lumen that cast posterior acoustic shadows, consistent with gallstones. The gallbladder wall is thin, measuring 0.28 cm, and the CBD is normal at 0.32 cm. There is no pericholecystic fluid, and the sonographic Murphy’s sign is negative. The stones are mobile when the patient’s position changes.
These findings support cholelithiasis without cholecystitis.
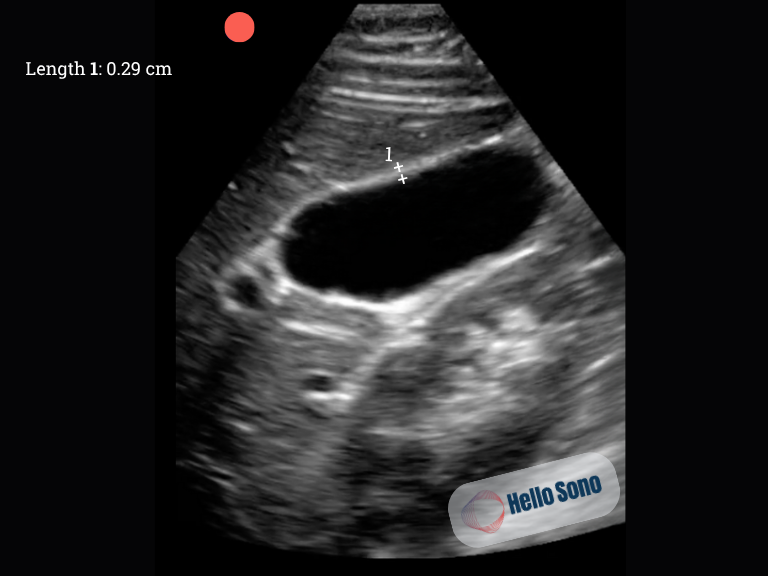
What a Normal POCUS Should Show
In a normal right upper quadrant ultrasound (Image 2), the gallbladder appears as an anechoic (black), pear-shaped structure with thin, smooth walls. There are no echogenic foci or posterior shadowing within the lumen. The CBD is typically less than 6 mm in diameter in patients under age 70. The anterior gallbladder wall measures less than 3 mm.
Evidence
For cholelithiasis, meta-analyses and large studies report POCUS sensitivity of 90–96% and specificity of 88–96%.[1-3] The most recent meta-analysis found a pooled sensitivity of 94% (95% CI: 91–96%) and specificity of 93% (95% CI: 91–95%) for gallstone detection.[1] This makes POCUS a reliable tool for ruling in or out gallstones in the emergency setting.
For acute cholecystitis, sensitivity is more variable due to the dynamic nature of the disease and reliance on secondary findings (wall thickening, pericholecystic fluid, sonographic Murphy’s sign). Pooled sensitivity in meta-analysis is 73% (95% CI: 55–86%) and specificity is 93% (95% CI: 82–98%).[1] Other studies report sensitivities ranging from 60% to 87%.[4-5]
Case Resolution
The provider diagnosed symptomatic cholelithiasis without evidence of cholecystitis or biliary obstruction. The patient was referred for an elective laparoscopic cholecystectomy and advised on dietary modification to avoid high-fat meals until surgical management.
Impact of POCUS
In this case, POCUS provided a rapid, radiation-free, and accurate diagnosis of gallstones during the patient’s office visit.
For primary care and urgent care providers, gallbladder POCUS can:
- Distinguish biliary colic from cholecystitis or other abdominal pain etiologies
- Identify complications such as choledocholithiasis through CBD assessment
- Support on-site decision-making and targeted referrals
- Improve patient satisfaction through immediate answers and visual confirmation
- Keep revenue in-house rather than referring out for imaging. Limited biliary ultrasound (CPT 76705) is reimbursed at approximately $84.10 under the 2025 Medicare physician fee schedule. Practices can estimate their potential reimbursement and financial impact using the POCUS ROI Calculators.
By integrating POCUS into the evaluation of right upper quadrant pain, clinicians can manage many abdominal pain presentations efficiently and safely in the outpatient setting.
Conclusion
This case highlights how bedside ultrasound enables the prompt diagnosis of symptomatic cholelithiasis in primary care, guiding appropriate referral for elective cholecystectomy. POCUS empowers primary care clinicians to deliver faster, evidence-based care, reduce reliance on radiology, and improve patient experience; all within the scope of routine office visits.
References:
- Wu X, Li K, Kou S, Wu X, Zhang Z. The Accuracy of Point-of-Care Ultrasound in the Detection of Gallbladder Disease: A Meta-analysis. Acad Radiol. 2024 Apr;31(4):1336-1343. doi: 10.1016/j.acra.2023.09.029. Epub 2023 Oct 12. PMID: 37838525.
- MacDonald AA, Richardson M, Sue L, Hakiwai A, Stephenson G, Harman R, Agraval J. Bedside ultrasonography for acute gallstone disease: a diagnostic accuracy study of surgical registrars and emergency medicine physicians. ANZ J Surg. 2020 Dec;90(12):2467-2471. doi: 10.1111/ans.16169. Epub 2020 Jul 31. PMID: 33216429.
- American College of Emergency Physicians. Emergency ultrasound guidelines. Ann Emerg Med. 2009 Apr;53(4):550-70. doi: 10.1016/j.annemergmed.2008.12.013. PMID: 19303521.
- Wehrle CJ, Talukder A, Tien L, Parikh S, Devarakonda A, Holsten SB, Fox ED, Lawson A. The Accuracy of Point-of-Care Ultrasound in the Diagnosis of Acute Cholecystitis. Am Surg. 2022 Feb;88(2):267-272. doi: 10.1177/0003134821989057. Epub 2021 Jan 31. PMID: 33517707.
- Gustafsson C, Lindelius A, Törngren S, Järnbert-Pettersson H, Sondén A. Surgeon-Performed Ultrasound in Diagnosing Acute Cholecystitis and Appendicitis. World J Surg. 2018 Nov;42(11):3551-3559. doi: 10.1007/s00268-018-4673-z. PMID: 29882098; PMCID: PMC6182762.